
Background
Child health and nutrition are key indicators of the country’s socioeconomic development and
quality of life. The purpose of the paper was to examine the level, trend, and socio-
demographic differences of selected child health and nutrition indicators and to provide policy
recommendations for improvement.
Methods
Desk review was conducted to compile secondary information on child health and nutrition
status published in the Nepal Demographic and Health Survey reports prepared by Ministry of
Health and Population from 1996 to 2016. Trend line, bar diagram, and GIS maps were
prepared to present the findings
Results
A substantial decrease in under-five mortality, from 118 to 39 (67% point decline) and
neonatal mortality, from 50 to 21 (57% point decline) deaths per 1000 live births, was noted
between 1996 and 2016. Full immunization coverage decreased to 78%, 36% of children
under the age of five were stunted, 25% were underweight, and 10% were wasted in 2016.
Boys were more likely to receive treatment for diarrhoea (72%), compared to girls (56%). The
majority of the children (74%) had their acute respiratory infections managed at private
medical centers. Child health and nutritional status differed by geographic regions, being
better in Gandaki and Bagmati and poor in Karnali and Madesh. Overall health and nutrition
status of children were better among educated, and wealthier families.
Conclusions
To further reduce childhood mortality and reach the targets for the Sustainable Development
Goal, targeted interventions must be implemented to improve immunization coverage plus
health and nutritional status among disadvantaged populations.
Keywords
Child Health, Child Mortality, Nepal, Nutritional Status
INTRODUCTION
The fundamental necessity of safeguarding and enhancing children’s health cannot be
overstated. Nepal has made significant advancements in recent decades in terms of children’s
health and mortality rates. To further enhance children’s health, much work still needs to be
done. One of the most crucial things for creating a better future for the Nepalese population is
to invest in children 1 . Since 1996, the Nepal Demographic and Health Survey (NDHS) has
been conducted every five years by the Ministry of Health and Population (MoHP) with
technical and financial support from the United States Agency for International Development
(USAID). The 2016 NDHS is the fifth round of this survey implemented in Nepal as part of
worldwide DHS 2 . This article aims to present the trend in childhood mortality, health and
nutrition status, and related socio-economic differences in Nepal and to provide policy
recommendations based on the NDHS data sets.
METHODS
We conducted a desk review of secondary information published in Nepal Demographic and
Health Survey (NDHS) reports prepared under the aegis of the Ministry of Health and
Population (MoHP) from 1996 to 2016 2-6 . These surveys used national population census data
as the basis for their sampling frames. Probability proportional to size sampling was used to
recruit a nationally representative sample of respondents and also produce provincial and
urban-rural estimates. These surveys used questionnaires for households, women, and men of
reproductive age to collect information on demographic and health issues. The questionnaires
were based on the standard Measure DHS questionnaire. The surveys obtained ethical
approval from Nepal Health Research Council (NHRC) and ICF international review board. A
response rate of more than 90% was achieved in all five surveys. Details of the survey design
and methodology and data set can be obtained from the DHS website, dhsprogram.com.
The key indicators examined in this report are childhood immunization, childhood illnesses
(diarrhoea, respiratory infection/ pneumonia) and related treatment-seeking behaviour,
childhood malnutrition, infant and young feeding practices, micronutrient supplementation,
breast-feeding and childhood mortality (neonatal, infant, child, and under-five mortality). The
indicators examined are presented in trend line and bar diagram using excel and the GIS maps
using QGIS software.
RESULTS
The results are presented here in four sections; childhood mortality, childhood immunization,
childhood illness, and childhood nutrition status respectively.
Childhood mortality
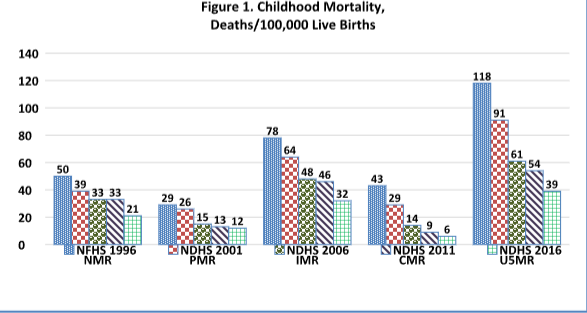
Over the twenty-year period between 1996 and 2016, all five childhood mortalities (neonatal,
perinatal, infant, child, and under-five) have gradually decreased. Figure1 indicates that the
neonatal mortality rate (NMR) has decreased to 21 per 1000 LB in 2016 from 50 per 1000 LB
in 1996 (a 58% point reduction; Annual Rate of Reduction, ARR- 2.9%). Similarly, the under-
five mortality rate (U5MR) decreased to 39 per 1000 LB in 2016 from 118 per 1000 LB in
1996 (a 67% point decrease; ARR-3.3%). This indicates that still, one in every 26 Nepali
children dies before their fifth birthday. To achieve the Sustainable Development Goal (SDG)
target by 2030, Nepal has to decrease the under-five mortality rate by 49% (at ARR of 3.5%)
and the neonatal mortality rate by 43% (at ARR of 3.1%) from the 2016 level. U5MR as well
as the other four childhood mortality rates also vary across provinces. Therefore, it is a
challenge for the Government of Nepal to remove the provincial-level disparity and to meet
the SDG targets of neonatal and under-five mortality set at 12 and 25 per 1000 LB,
respectively. This calls for an urgent need to accelerate the implementation of targeted
interventions 7 .
Childhood immunization
Immunization is the most cost-effective and efficient way to control and eliminate the
vaccine-preventable diseases that contribute to childhood illness and deaths 2 . All children in
Nepal need to be vaccinated with the recommended number of doses of BCG, DPT-HepB-
HIB, OPV, PCV, IPV-IM, and measles/rubella vaccine during the first year of life 8 . Over the
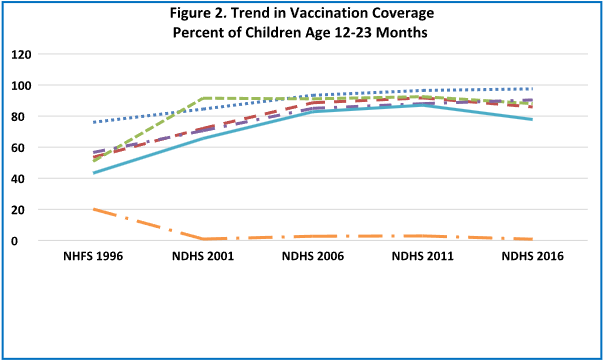
last two decades, full immunization coverage in Nepal has increased from 43% in 1996 to
78% in 2016 (81.4% point increase; annual rate of increase, ARI-4%) however, the full
immunization coverage has declined by almost 10% point (from 87% in 2011 to 78% in 2016)
(Figure 2). Full immunization coverage also varied across provinces (highest in Gandaki-
93%) and lowest in Madhesh (65%) 2 . To meet the SDG target of full immunization (95% by
2030), Nepal has to increase the full immunization coverage by the annual rate of increase
(ARI) of 1.5% during 2016-2030. Parental education can play an important role to achieve the
target, because, full immunization coverage among children aged 12-23 months increased in
Nepal with the mother’s education (68% among uneducated mothers and 91% among mothers
with SLC or higher education) 2 . Even after taking other indicators of the family’s
socioeconomic condition into account, lower maternal and father education are both risk
factors for child health and mortality as documented in a global systematic review and meta-
analysis 9 .
Childhood illness: Diarrhoea
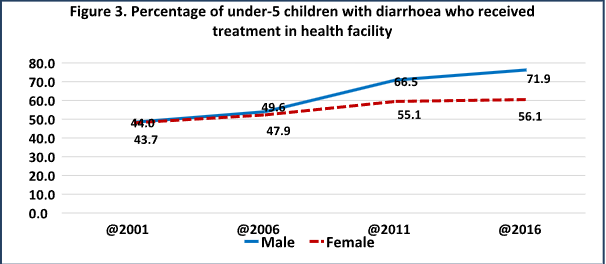
Nepal has experienced an impressive reduction in the prevalence of diarrhoea among under-
five children (from 21.3% in 2001 to 7.7% in 2016 among males and from 19.5% to 7.5%
among females) 2-5 but only 72% of male children and 56% of female children sought treatment
from health facilities (Figure 3) and 16% children did not get any treatment (even oral
rehydration solution, ORS). As diarrhoea is one of the major killers of under-5 mortality,
appropriate intervention to timely bring the patient for treatment in a health facility using
modern technology is very important for reducing childhood mortality due to diarrhoea.
Childhood illness: ARI/Pneumonia
The prevalence of ARI among children under-five in Nepal decreased from 5% in 2011 to 2%
in 2016 (a 60% reduction), however, ARI and Pneumonia are still a major public health
problem and a leading cause of death among these children 2-3 . In 2016, ARI prevalence is the
highest among children aged 6-23 months (8%) and decreased with household wealth (3%
among children living in a household with the bottom two wealth quintile and 1% in the
highest wealth quintile) and varies across provinces and educational status of mothers 2 .
Treatment for ARI was most commonly sought from a private medical store (74%) and only
23% were taken to government facilities. To further reduce the prevalence of ARI and
Pneumonia, advocacy, particularly among poor, uneducated and hard-to-reach group is
required to bring them to health facilities for early treatment.
Childhood nutrition status
Nutrition status is primarily determined by a child’s growth in height and weight and is
directly influenced by food intake and the occurrence of infections 10 . Weight-for-age is a
composite index of weight-for-height and height-for-age. Both acute (wasting) and chronic
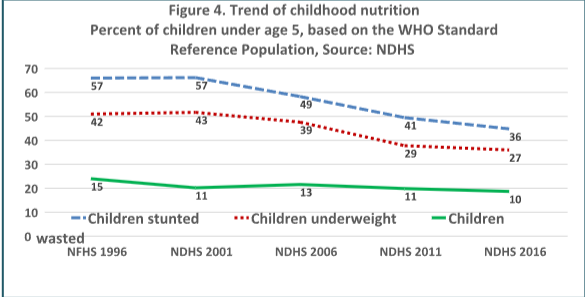
(stunting) occur as an indicator of overall nutrition 2 . More than one-third (36%) of children
under five-year age were stunted, one in every ten (10%) children were wasted and slightly
more than a quarter (27%) of children were underweight in 2016 2 . The prevalence of stunting
substantially decreased from 57% in 1996 to 96% in 2016 (37% point decline; ARR-1.9%),
similarly, the prevalence of underweight declined from 42% to 27% (36% decline; ARR-
1.8%) during the same period, however, the prevalence of wasting remained same (around
10%) during 2001 to 2016 (Figure 4). Chronic malnutrition is most prevalent in Karnali
province (55%), Lumbini province (39%), and Madhesh (37%) and it is lowest in Gandaki
and Bagmati provinces (29%). Globally, inequalities within a nation have frequently been
associated with inverse relationships between child mortality and socioeconomic level 11-13 .
Children of uneducated mothers and those living in poorer households suffer more than
educated and wealthier families. The average ARR of stunting and underweight over 20 year
period between 1996 to 2016 were 1.9% and 1.8% respectively, which are much lower than
the required 4.2% and 5.8% ARR respectively during 2016-2030. Therefore, Nepal is less
likely to achieve the SDG target for reducing childhood stunting, underweight, and wasting in
Nepal.
Anaemia among children is a condition marked by a low level of haemoglobin in red blood
cells. Iron is a key component of haemoglobin and iron deficiency is known to be responsible
for half of all anaemia globally. Malaria, hookworm, chronic infection, blood disorder, and
genetic condition are well-known causes of anaemia 2 . Anaemia is a serious concern for
children because it impairs their development with associated longterm health and economic
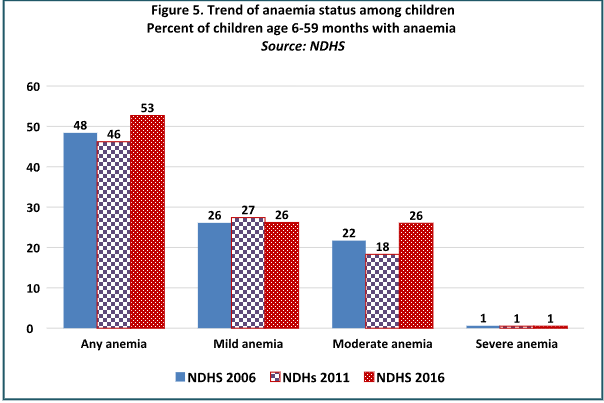
consequence and leads to increased mortality 2 . The prevalence of anaemia among children 6-
59 months is 53% with 26% mildly anaemic, 26% moderately anaemic and 1% severely
anaemic in 2016 in Nepal (Figure 5). Prevalence of anaemia among children under age 5
declined by 2% point from 2006 to 2011. But it increased by 7% points (from 46% in 2011 to
53% in 2016). Over the past 5 years, the prevalence of mild and severe anaemia have been
almost stagnant, while notable increase in moderate anaemia was observed (from 18% to
26%) (Figure 5). Prevalence of anaemia was higher in rural (56%) compared with urban
(49%). Similarly, the prevalence of anaemia was highest in Madhesh province (59%) and
Bagmati province had lowest anaemia prevalence (43%) in 2016. Focused interventions
associated with quality education and poverty reduction activities are required to improve the
childhood anaemia status in Nepal.
DISCUSSION
Measures of infant and child health and mortality status are sensitive indices of the health and
happiness of a population because they take into account a variety of individual, mother,
household, community, and environmental factors 14-16 . This paper presents the trend of child
health and nutrition status using NDHS data. Specifically, childhood mortality, immunization,
respiratory illness, diarrhoea and nutrition status as well as their differentials across the
population are examined and policy recommendations to improve child health and nutrition
status are provided. The evidence show that under-five and neonatal mortalities are decreasing
at the annual rate of 3.3% and 2.9% respectively in Nepal. This rate of reduction should be
increased to meet the SDG target.
Common causes of neonatal mortality are infection, birth asphyxia and prematurity and under-
five mortality are respiratory infections, diarrhoea, malaria and birth complications.
Therefore, it is essential to make sure that every pregnant mother and newborn get access to
life-saving interventions in order to increase neonatal survival 17-19 . Expanding birthing centres
(BC) at strategic location of remote and hard-to-reach areas and making them function is very
important to substantially increase institutional delivery. Implementation of well-known
newborn interventions such as the application of chlorhexidine for cord care, resuscitation for
newborns, management of newborn infection, use of antenatal corticosteroids and kangaroo
mother care are needed to accelerate childhood mortality reduction. Reinforcing behaviour
change communication through various channels to improve parenting skills for newborn
care, particularly among the poor, uneducated, minority and hard-to-reach population are
urgently required 20 .
Full immunization is key to child survival and missing routine immunization can be life-
threatening to infants and children. However, full immunization coverage is in declining trend
in Nepal. To attain the SDG target, full immunization coverage has to be increased at the rate
of 1.5% per year. Therefore, MoHP should implement innovative interventions to accelerate
full immunization. Working closely with development partners and other government
stakeholders to narrow the full immunization gaps, particularly among poor, marginalized and
less educated groups in all geographical areas should be a key focus. Ensuring the availability
of uninterrupted vaccines and motivated vaccinators supported by community awareness on
the benefit of vaccination timing and place of vaccination and integrating immunization
programs with other maternal and newborn programs can be a helpful strategy to increase full
immunization and reduce disparity across socio-demographic groups 21 .
Despite decreasing trend of diarrhoea prevalence in Nepal, the treatment-seeking behaviour is
not very impressive. The primary cause of death in children under the age of five is diarrhoea,
which can be made worse by micronutrient deficiency. The severity of diarrhoea is lessened
by vitamin A supplementation given every six months, but the overall morbidity linked to
diarrhoea is unaffected. It has been demonstrated that regular zinc supplementation lowers the
prevalence and mortality of diarrhoea 22 . Exploring further to examine reasons for poor
treatment of diarrhoea and developing a strategy towards achieving universal use of ORS for
the treatment of diarrhoeal diseases is of utmost importance. The interventions related to the
universal use of ORS should be focused on female, uneducated and poor households.
Improving access to medicine (ORS, Zinc and antibiotics, etc.), food, and clean water as well
as public education through health workers and community health volunteers (CHV) can save
lives.
Treatment of ARI and pneumonia using antibiotics is the key strategy for preventing death
due to respiratory diseases, but excessive use of antibiotics might have an adverse effect on
the health of children 23 . Regulating the uncontrolled use of antibiotics to prevent children from
developing antibiotic resistance requires the adoption of effective approaches. As a low birth
weight, malnutrition, and lack of breast-feeding are important risk factors for childhood ARI
and pneumonia, nutritional interventions such as early and exclusive breastfeeding,
vaccination, access to clean water, good nutrition and limited exposure to air pollution should
be implemented to reduce deaths from ARI and pneumonia 24 .
A supply of trained health workers equipped with adequate medicines and equipment within easy reach of poor and uneducated families are helpful to treat childhood ARI and pneumonia effectively.
The NDHS reports also show that the nutrition status of Nepalese children is poor. More than
one-third of children under the age of five are stunted. Although the prevalence of stunting
has been decreased at the annual rate of 1.9%, to meet the SDG target, the annual rate of
reduction in stunting and underweight should be over 4.2% and 5.8% respectively. Residents
of Karnali and Madhesh Province, poor, and uneducated families are more vulnerable to
undernutrition. Exclusive breastfeeding, complementary feeding, micronutrient
supplementations, adequate and balanced diet during pregnancy, and treatment of acute
malnutrition are the potential nutrition-specific interventions that have a direct impact on the
nutrition status of children 23 . Increasing the coverage of nutrition-specific interventions listed
above across the population through both public and non-government (NGO) sectors can be
immensely important to improve nutrition status.
Counselling mothers effectively to improve child feeding practices and disseminating
messages about good child feeding practices on cell phones, radio and television help its
promotion. Appropriate community-based interventions for children with severe acute
malnutrition should be implemented. Calcium supplementation during pregnancy is
documented to be helpful to prevent pre-eclampsia, eclampsia and gestational hypertension
which in turn provides better maternal and foetal outcomes and should be a nationwide
implementation. Implementing nutrition-specific interventions together with nutrition-
sensitive interventions (such as food security, family planning, proper water, sanitation and
hygiene, and women’s empowerment), particularly for uneducated, poor and vulnerable
children is helpful to substantially reduce stunting. Multi-sectoral collaboration, deployment
of trained staff in the community, and effective communication for changing the behaviour of
vulnerable people are key to improving the nutritional status of children 25 .
CONCLUSIONS
Nepalese children are living healthier lives than ever before. Neonatal, infant and child
mortality continues to decrease, child vaccination is slowly rising, and fewer children are
malnourished. However, Nepal still lags behind its neighbours in South Asia in many of the
key indicators. Greater effort is therefore required to meet the SDG target of child health and
nutrition indicators. Targeted interventions must be made to improve immunization coverage
and nutritional status among disadvantaged populations.
ACKNOWLEDGEMENT
The authors would like to thank Ministry of Health and Population and ICF International Inc.
for giving approval to use the NDHS data sets.
REFERENCES
- Child health [Internet]. www.who.int. Available from: https://www.who.int/health-
topics/child-health - Ministry of Health, Nepal; New ERA; and ICF. Nepal Demographic and Health Survey
- Kathmandu, Nepal: Ministry of Health, Nepal; 2017. Accessed online from:
https://dhsprogram.com/pubs/pdf/FR336/FR336.pdf. - Ministry of Health and Population (MOHP) [Nepal], New ERA, and ICF International Inc.
- Nepal Demographic and Health Survey 2011. Kathmandu, Nepal: Ministry of Health
and Population, New ERA, and ICF International, Calverton, Maryland. Accessed online from
https://dhsprogram.com/pubs/pdf/fr257/fr257%5B13april2012%5D.pdf. - Ministry of Health and Population (MOHP) [Nepal], New ERA, and Macro International
Inc. 2007. Nepal Demographic and Health Survey 2006. Kathmandu, Nepal: Ministry of
Health and Population, New ERA, and Macro International Inc. Accessed online from
https://dhsprogram.com/pubs/pdf/FR191/FR191.pdf. - Ministry of Health [Nepal], New ERA, and ORC Macro. 2002. Nepal Demographic and
Health Survey 2001. Calverton, Maryland, USA: Family Health Division, Ministry of Health;
New ERA; and ORC Macro. Accessed online from
https://dhsprogram.com/pubs/pdf/fr132/fr132.pdf. - Pradhan, Ajit, Ram Hari Aryal, Gokarna Regmi, Bharat Ban, and Pavalavalli
Govindasamy. 1997. Nepal Family Health Survey 1996. Kathmandu, Nepal and Calverton,
Maryland: Ministry of Health [Nepal], New ERA, and Macro International Inc. Accessed
online from https://dhsprogram.com/pubs/pdf/fr78/fr78.pdf. - National Planning Commission (NPC). Sustainable Development Goals Status and
Roadmap: 2016-2030. Singhadurbar, Kathmandu, Nepal: National Planning Commission; - Available from: https://www.undp.org/nepal/publications/sustainable-development-
goals-status-and-roadmap-2016-2030# - Department of Health Services (DoHS). Annual Health Report 2076/77 (2019/2020). Teku,
Kathmandu, Nepal: Department of Health Services; 2020. Available from:
- Balaj M, York HW, Sripada K, Besnier E, Vonen HD, Aravkin A, et al. Parental education
and inequalities in child mortality: a global systematic review and meta-analysis. The Lancet.
2021 Aug 14;398(10300):608-20. Available from: [Article] - ICF International. Children’s Health and Nutritional Status: Data from the 2011 Ethiopia
Demographic and Health Survey. Calverton, Maryland, USA: ICF International; 2012.
Available from: https://dhsprogram.com/pubs/pdf/DM25/DM25.pdf. - Gwatkin DR. Health inequalities and the health of the poor: what do we know? What can
we do?. Bulletin of the world health organization. 2000;78:3-18. Available from: [PubMed] - Adler NE, Ostrove JM. Socioeconomic status and health: what we know and what we
don’t. Annals of the New York academy of Sciences. 1999 Dec;896(1):3-15. Available from:
[PubMed] - Houweling TA, Kunst AE. Socio-economic inequalities in childhood mortality in low-and
middle-income countries: a review of the international evidence. British medical bulletin.
2010 Mar 1;93(1):7-26. Available from: [PubMed] - Mosley WH, Chen LC. An analytical framework for the study of child survival in
developing countries. Population and development review. 1984 Jan 1;10:25-45. Available
from: [PubMed] - Victora CG, Wagstaff A, Schellenberg JA, Gwatkin D, Claeson M, Habicht JP. Applying
an equity lens to child health and mortality: more of the same is not enough. The Lancet. 2003
Jul 19;362(9379):233-41. Available from: [Article] - Van de Poel E, O’donnell O, Van Doorslaer E. What explains the rural-urban gap in infant
mortality: household or community characteristics?. Demography. 2009 Nov;46(4):827-50.
Available from: [PubMed] - Bhutta ZA, Das JK, Bahl R, Lawn JE, Salam RA, Paul VK, Sankar MJ, Blencowe H,
Rizvi A, Chou VB, Walker N. Can available interventions end preventable deaths in mothers,
newborn babies, and stillbirths, and at what cost?. The Lancet. 2014 Jul 26;384(9940):347-70.
Available from: [PubMed] - Darmstadt GL, Bhutta ZA, Cousens S, Adam T, Walker N, De Bernis L, Lancet Neonatal
Survival Steering Team. Evidence-based, cost-effective interventions: how many newborn
babies can we save?. The Lancet. 2005 Mar 12;365(9463):977-88. Available from: [PubMed] - Lassi ZS, Bhutta ZA. Community‐based intervention packages for reducing maternal and
neonatal morbidity and mortality and improving neonatal outcomes. Cochrane database of
systematic reviews. 2015(3). Available from: [PubMed] - Olack, B., Santos, N., Inziani, M., Moshi, V. et al. (2021). Causes of preterm and low
birth weight neonatal mortality in a rural community in Kenya: evidence from verbal
and social autopsy. BMC Pregnancy Childbirth (2021) 21:536 https://doi.org/10.1186/s12884-
021-04012-z - Maternal and Neonatal Immunization Field Guide for Latin America and the Caribbean.
Washington, D.C. : PAHO; 2017. - Fischer Walker CL, Black RE. Micronutrients and diarrheal disease. Clinical infectious
diseases. 2007 Jul 15;45(Supplement_1):S73-7. Available from: [PubMed] - National Institute of Population Research and Training (NIPORT) and ICF International.
Bangladesh Demographic and Health Survey 2014: Policy Briefs. Dhaka, Bangladesh and
Rockville, Maryland, USA: NIPORT and ICF International; 2016. Available from:
https://dhsprogram.com/pubs/pdf/FR311/FR311.pdf - Victoria, C.G., Kirkwood, B.R., Ashworth, A., Black, R. E., Rogers, S., Sazawal, S.,
Campbell, H., and Gove, S. (1999). Potential interventions for the prevention of childhood
pneumonia in developing countries: improving nutrition. Am J Clin Nutr 1999; 70:309–20.
Available from: [PubMed] - National Institute of Population Research and Training (NIPORT) and ICF International.
(2016). Bangladesh Demographic and Health Survey 2014: Policy Briefs. Dhaka, Bangladesh
and Rockville, Maryland, USA: NIPORT and ICF International.
Legends
Table
Figures
Figure 1. Childhood mortality (Deaths/100,000 LB)
Figure 2. Trend in vaccination coverage (Percent of children age 12-23 months)
Figure 3. Percentage of under-5 children with diarrhoea who received treatment in health
facility
Figure 4. Trend of childhood nutrition (Percent of children under age 5 based on the WHO
standard reference population)
Figure 5. Trend of anemia status among children